
Oxidative Stress in Structural Valve Deterioration: A Longitudinal Clinical Study

 , , , , , , add
Show full author list
, , , , , , add
Show full author list
Abstract
:1. Introduction
2. Patients and Methods
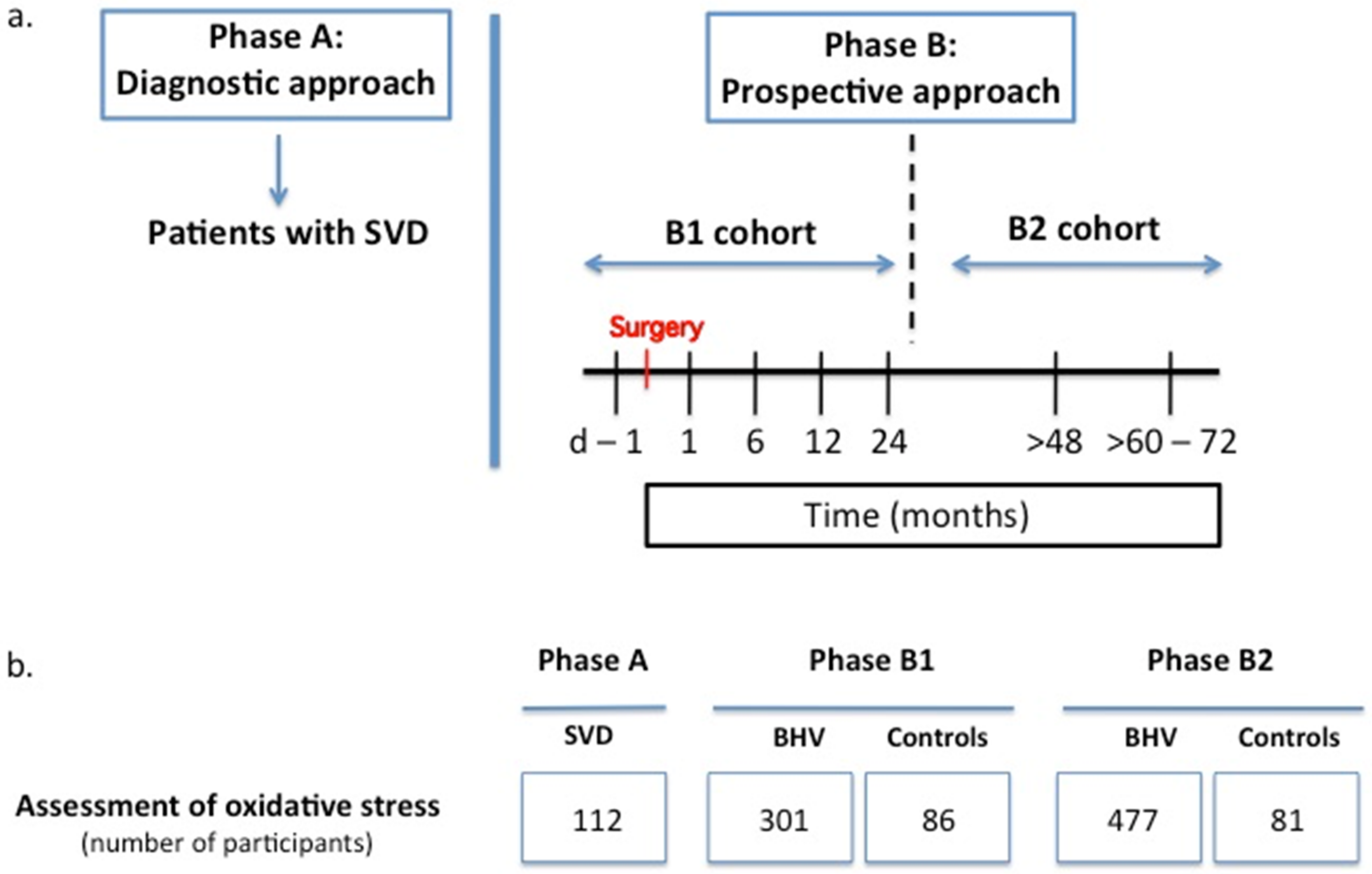
2.1. Study Population
2.2. Study Protocol
2.3. Procurement of Samples and Informed Consent
2.4. Echocardiographic Assessment and Definition of Structural Valve Disease (SVD)
2.5. Assessment of Total Antioxidant Capacity (TAC)
2.6. Assessment of Malondialdehyde (MDA)
2.7. Assessment of Nitrotyrosine (NT)
2.8. Statistical Analyses
3. Results
3.1. Oxidative Stress during the First 24 Months after BHV Implantation (Phase B1)
3.2. Oxidative Stress in Incipient SVD (Phase B1)
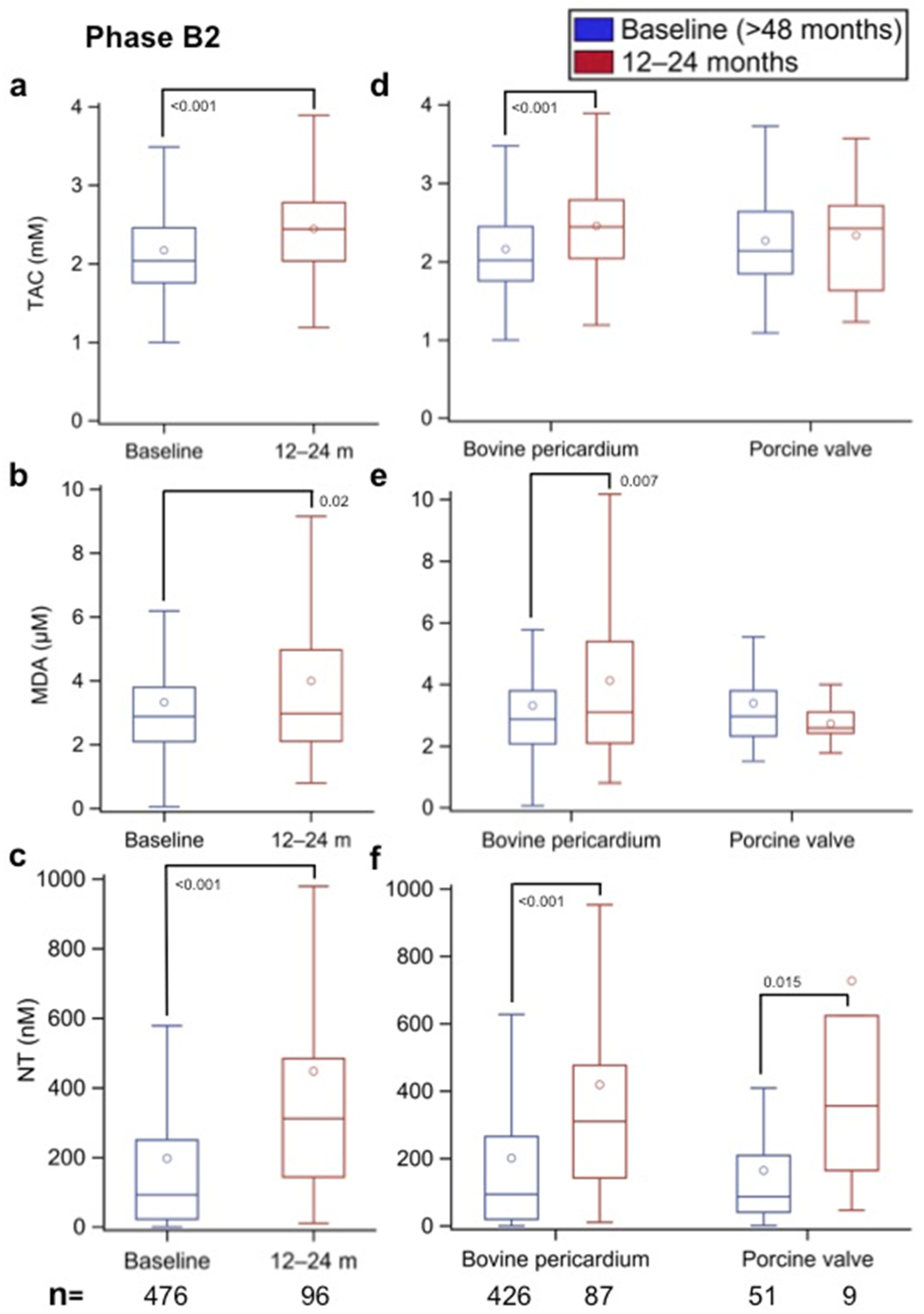
3.3. Oxidative Stress Associated with SVD (Phase A) and BHVs >48 Months after AVR (Phase B2)
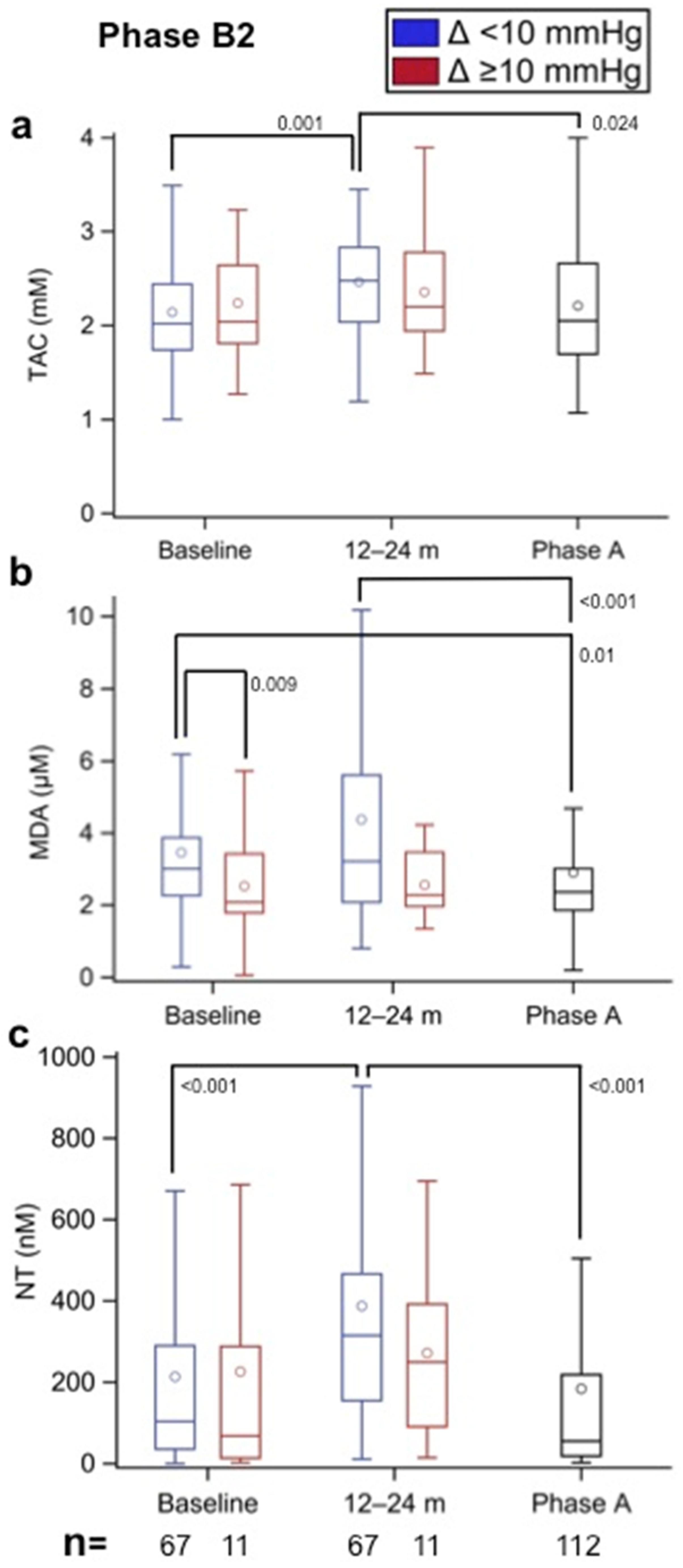
3.4. Oxidative Stress Changes in the Follow-Up of Phase B2 Patients
3.5. Effect of the Source of BHV Tissue on Oxidative Stress (Phase B2)
3.6. Oxidative Stress in Incipient SVD (Phase B2)
3.7. Effect of BHV Framework Type and Size on Oxidative Stress (Phase B2)
3.8. Effect of Comorbidities and Medical Treatments on Oxidative Stress
4. Discussion
4.1. Oxidative Stress Increases after BHV Implantation and Decreases Once SVD Develops
4.2. Oxidative Stress Is Greater in TAVI Patients
4.3. Influence of BHV Tissue Type and Size on Oxidative Stress
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pibarot, P.; Dumesnil, J.G. Prosthetic heart valves: Selection of the optimal prosthesis and long-term management. Circulation 2009, 119, 1034–1048. [Google Scholar] [CrossRef] [PubMed]
- Sénage, T.; Gillaizeau, F.; Le Tourneau, T.; Marie, B.; Roussel, J.C.; Foucher, Y. Structural valve deterioration of bioprosthetic aortic valves: An understimated complication. J. Thorac. Cardiovasc. Surg. 2019, 157, 1383–1390. [Google Scholar] [CrossRef] [PubMed]
- Chiang, Y.P.; Chikwe, J.; Moskowitz, A.J.; Itagaki, S.; Adams, D.H.; Egorova, N.N. Survival and long-term outcome following bioprosthetic vs mechanical aortic valve replacement in patients aged 50 to 69 years. JAMA 2014, 312, 1323–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capodanno, D.; Petronio, A.S.; Prendergast, B.; Eltchaninoff, H.; Vahanian, A.; Modine, T.; Lancellotti, P.; Sondergaard, L.; Ludman, P.F.; Tamburino, C.; et al. Standardized definitions of structural deterioration and valve failure in assessing long-term durability of transcatheter and surgical aortic bioprosthetic valves: A consensus statement from the European Association of Percutaneous Cardiovascular Interventions (EAPCI) endorsed by the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2017, 38, 3382–3390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dvir, D.; Bourguignon, T.; Otto, C.M.; Hahn, R.T.; Rosenhek, R.; Webb, J.G.; Treede, H.; Sarano, M.E.; Feldman, T.; Wijeysundera, H.C.; et al. On behalf of VIVID (Valve in Valve International Data) investigators. Standardized definition of structural valve degeneration for surgical and transcatheter bioprosthetic aortic valves. Circulation 2018, 137, 388–399. [Google Scholar] [CrossRef]
- Sénage, T.; Le Tourneau, T.; Foucher, Y.; Pattier, S.; Cueff, C.; Michel, M.; Serfaty, J.M.; Mugniot, A.; Périgaud, C.; Carton, H.F.; et al. Early structural valve deterioration of Mitroflow aortic bioprosthesis: Mode, incidence, and impact on outcome in a large cohort of patients. Circulation 2014, 130, 2012–2020. [Google Scholar] [CrossRef]
- Sabbah, H.N.; Hamid, M.S.; Stein, P.D. Mechanical factors in the degeneration of porcine bioprosthetic valves: An overview. J. Card. Surg. 1989, 4, 302–309. [Google Scholar] [CrossRef]
- Coté, N.; Mahmut, A.; Bosse, Y.; Couture, C.; Pagé, S.; Trahan, S.; Boulanger, M.C.; Fournier, D.; Pibarot, P.; Mathieu, P. Inflammation is associated with the remodeling of calcific aortic valve disease. Inflammation 2013, 36, 573–581. [Google Scholar] [CrossRef]
- Mangold, A.; Szerafin, T.; Hoetzenecker, K.; Hacker, S.; Lichtenauer, M.; Niederpold, T.; Nickl, S.; Dworschak, M.; Blumer, R.; Auer, J.; et al. Alpha-Gal specific IgG immune response after implantation of bioprostheses. Thorac. Cardiovasc. Surg. 2009, 57, 191–195. [Google Scholar] [CrossRef]
- Senage, T.; Paul, A.; Le Tourneau, T.; Fellah-Hebia, I.; Vadori, M.; Bashir, S.; Galiñanes, M.; Bottio, T.; Gerosa, G.; Evangelista, A.; et al. Early antibody responses against glycans of bioprosthetic heart valves support their eventual calcification. Nat. Med. 2022, 28, 283–294. [Google Scholar] [CrossRef]
- Flameng, W.; Herregods, M.C.; Vercalsteren, M.; Herijgers, P.; Bogaerts, K.; Meuris, B. Prosthesis-patient mismatch predicts structural valve degeneration in bioprosthetic heart valves. Circulation 2010, 121, 2123–2129. [Google Scholar] [CrossRef] [Green Version]
- Blasco-Lucas, A.; Permanyer, E.; Pérez, M.L.; Gracia-Baena, J.M.; Rios, R.; Casós, K.; Galiñanes, M. Effect of bioprostheses anti-calcification treatment: Comparative follow-up between mitroflow LX and Magna pericardial xenografts using propensity score-weighted analysis. Interact. Cardiovasc. Thorac. Surg. 2017, 24, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Naso, F.; Gandaglia, A.; Bottio, T.; Tarzia, V.; Nottle, M.B.; d’Apice, A.J.F.; Cowan, P.J.; Cozzi, E.; Galli, C.; Lagutina, I.; et al. First quantification of alpha-Gal epitope in current glutaraldehyde-fixed heart valve bioprostheses. Xenotransplantation 2013, 20, 252–261. [Google Scholar] [CrossRef]
- Reuven, E.M.; Leviatan Ben-Arye, S.; Marshanski, T.; Breimer, M.E.; Yu, H.; Fellah-Hebia, I.; Roussel, J.C.; Costa, C.; Galiñanes, M.; Mañez, R.; et al. Characterization of immunogenic Neu5Gc in bioprosthetic heart valves. Xenotransplantation 2016, 23, 381–392. [Google Scholar] [CrossRef] [Green Version]
- Mirzaie, M.; Meyer, T.; Saalmüller, A.; Dalichau, H. Influence of glutaraldehyde fixation on the detection of SLA-I and II antigens and calcification tendency in porcine cardiac tissue. Scand. Cardiovasc. J. 2000, 34, 589–592. [Google Scholar] [CrossRef]
- Liberman, M.; Bassi, E.; Martinatti, M.K.; Lario, F.C.; Wosniak, J., Jr.; Pomerantzeff, P.M.A.; Laurindo, F.R.M. Oxidant generation predominates around calcifying foci and enhances progression of aortic valve calcification. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 463–470. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.D.; Chu, Y.; Brooks, R.M.; Richenbacher, W.E.; Pena-Silva, R.; Heistad, D.D. Dysregulation of antioxidant mechanisms contributes to increased oxidative stress in calcific aortic valvular stenosis in humans. J. Am. Coll. Cardiol. 2008, 52, 843–850. [Google Scholar] [CrossRef] [Green Version]
- Towler, D.A. Oxidation, inflammation, and aortic valve calcification peroxide paves an osteogenic path. J. Am. Coll. Cardiol. 2008, 52, 851–854. [Google Scholar] [CrossRef] [Green Version]
- Olsson, M.G.; Allhorn, M.; Bulow, L.; Hansson, S.R.; Ley, D.; Olsson, M.L.; Schmidtchen, A.; Åkerström, B. Pathological conditions involving extracellular hemoglobin: Molecular mechanisms, clinical significance, and novel therapeutic opportunities for α-1-microglobulin. Antioxid. Redox Signal. 2012, 17, 813–846. [Google Scholar] [CrossRef] [Green Version]
- Christian, A.J.; Lin, H.; Alferiev, I.S.; Connolly, J.M.; Ferrari, G.; Hazen, H.; Ischiropoulos, H.; Levy, R.J. The susceptibility of bioprosthetic heart valve leaflets to oxidation. Biomaterials 2014, 35, 2097–2102. [Google Scholar] [CrossRef]
- Lee, S.; Levy, R.J.; Christian, A.J.; Hazen, S.L.; Frick, N.E.; Lai, E.K.; Grau, J.B.; Bavaria, J.E.; Ferrari, G. Calcification and oxidative modifications are associated with progressive bioprosthetic heart valve dysfunction. JAHA 2017, 6, e005648. [Google Scholar] [CrossRef] [PubMed]
- Fatouros, I.G.; Jamurtas, A.Z.; Villiotou, V.; Pouliopoulou, S.; Fotinakis, P.; Taxildaris, K.; Deliconstantinos, G. Oxidative stress responses in older men during endurance training and detraining. Med. Sci. Sports Exerc. 2004, 36, 2065–2072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrocco, I.; Altieri, F.; Peluso, I. Measurement and clinical significance of biomarkers of oxidative stress in humans. Oxid. Med. Cell. Longev. 2017, 2017, 6501046. [Google Scholar] [CrossRef] [PubMed]
- Mohty, D.; Pibarot, P.; Després, J.P.; Côté, C.; Arsenault, B.; Cartier, A.; Cosnay, P.; Couture, C.; Mathieu, P. Association between plasma LDL particle size, valvular accumulation of oxidized LDL, and inflammation in patients with aortic stenosis. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 187–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Côté, C.; Pibarot, P.; Després, J.P.; Mohty, D.; Cartier, A.; Arsenault, B.J.; Couture, C.; Mathieu, P. Association between circulating oxidised low-density lipoprotein and fibrocalcific remo-delling of the aortic valve in aortic stenosis. Heart 2008, 94, 1175–1180. [Google Scholar] [CrossRef]
- Valerio, V.; Myasoedova, V.A.; Moschetta, D.; Porro, B.; Perrucci, G.L.; Cavalca, V.; Cavallotti, L.; Songia, P.; Poggio, P. Impact of oxidative stress and protein S-glutathionylation in aortic valve sclerosis patients with overt atherosclerosis. J. Clin. Med. 2019, 8, 552. [Google Scholar] [CrossRef] [Green Version]
- Parhami, F.; Morrow, A.D.; Balucan, J.; Leitinger, N.; Watson, A.D.; Tintut, Y.; Berliner, J.A.; Demer, L.L. Lipid oxidation products have opposite effects on calcifying vascular cell and bone cell differentiation. A possible explanation for the paradox of arterial calcification in osteoporotic patients. Arterioscler. Thromb. Vasc. Biol. 1997, 17, 680–687. [Google Scholar] [CrossRef]
- Johnson, R.C.; Leopold, J.A.; Loscalzo, J. Vascular calcification: Pathobiological mechanisms and clinical implications. Circ. Res. 2006, 99, 1044–1059. [Google Scholar] [CrossRef] [Green Version]
- Matata, B.M.; Galiñanes, M. Cardiopulmonary bypass exacerbates oxidative stress but does not increase proinflammatory cytokines release in diabetics compared with non-diabetic patients: Regulatory effects of exogenous nitric oxide. J. Thorac. Cardiovasc. Surg. 2000, 120, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Matata, B.M.; Galiñanes, M. Off-pump bypass graft surgery significantly reduces oxidative stress and inflammation. Ann. Thorac. Surg. 2000, 69, 785–791. [Google Scholar] [CrossRef]
- Wu, J.H.Y.; Marchioli, R.; Silletta, M.G.; Masson, S.; Selke, F.W.; Libby, P.; Milne, G.L.; Brown, N.J.; Lombardi, F.; Damiano, R.J., Jr.; et al. Oxidative stress biomarkers and incidence of postoperative atrial fibrillation in the omega-3 fatty acids for prevention of postoperative atrial fibrillation (OPERA) trial. JAHA 2015, 4, e001886. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, A.; Chowdhury, S.; Bhattacharyy, M. Effect of metformin on oxidative stress, nitrosative stress and inflammatory biomarkers in type 2 diabetes patients. Diabetes Res. Clin. Pract. 2010, 93, 56–62. [Google Scholar] [CrossRef]
- Hou, X.; Song, J.; Li, X.-N.; Zhang, L.; Wang, X.L.; Chen, L.; Shen, Y.H. Metformin reduces intracellular reactive oxygen species levels by upregulating expression of the antioxidant thioredoxin via the AMPK-FOXO3 pathway. Biochem. Biophys. Res. Commun. 2010, 396, 199–205. [Google Scholar] [CrossRef]
- Findeisen, K.; Morticelli, L.; Goecke, T.; Kolbeck, L.; Ramm, R.; Höffler, H.K.; Brandes, G.; Korossis, S.; Haverich, A.; Hilfiker, A. Toward acellular xenogeneic heart valve prostheses: Histological and biomechanical characterization of decellularized and enzymatically deglycosylated porcine pulmonary heart valve matrices. Xenotransplantation 2020, 27, e12617. [Google Scholar] [CrossRef]
- Crockett-Torabi, E.; Fantone, J.C. Soluble and insoluble immune complexes activate human neutrophil NADPH oxidase by distinct Fcγ receptor-specific mechanisms. J. Immunol. 1990, 145, 3026–3032. [Google Scholar]
- Nimmerjahn, F.; Ravetch, J.V. Fcgamma receptors as regulators of immune responses. Nat. Rev. Immunol. 2008, 8, 34–47. [Google Scholar] [CrossRef]
- Kim, M.S.; Jeong, S.; Lim, H.G.; Kim, Y.J. Differences in xenoreactive immune response and patterns of calcification of porcine and bovine tissues in α-Gal knock-out and wild-type mouse implantation models. Eur. J. Cardiothorac. Surg. 2015, 48, 392–399. [Google Scholar] [CrossRef] [Green Version]
- Perota, A.; Lagutina, I.; Duchi, R.; Zanfrini, E.; Lazzari, G.; Judor, J.P.; Conchon, S.; Bach, J.M.; Bottio, T.; Gerosa, G.; et al. Generation of cattle knockout for galactose-α1,3-galactose and N-glycolylneuraminic acid antigens. Xenotransplantation 2019, 26, e12524. [Google Scholar] [CrossRef]
- Salama, A.; Mosser, M.; Lévêque, X.; Perota, A.; Judor, J.P.; Danna, C.; Pogu, S.; Mouré, A.; Jégou, D.; Gaide, N.; et al. Neu5Gc and α1-3 GAL xenoantigen knockout does not affect glycemia homeostasis and insulin secretion in pigs. Diabetes 2017, 66, 987–993. [Google Scholar] [CrossRef] [Green Version]
- Alavi, S.; Groves, E.M.; Kheradvar, A. The effects of transcatheter valve crimping on pericardial leaflets. Ann. Thorac. Surg. 2014, 97, 1260–1266. [Google Scholar] [CrossRef] [Green Version]
- Zareian, R.; Tseng, J.C.; Fraser, R.; Meganck, J.; Kilduff, M.; Sarraf, M.; Dvir, D.; Kheradvar, A. Effect of stent crimping on calcification of transcatheter aortic valves. Interact. Cardiovasc. Thorac. Surg. 2019, 29, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Ramm, C.J.; Misenheimer, J.A.; Vavalle, J.P. Early transcatheter valve prosthesis degeneration and future ramifications. Cardiovasc. Diagn. Ther. 2017, 7, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Jose, J.; Sulimov, D.; El-Mawardy, M.; Sato, T.; Allali, A.; Holy, E.W.; Becker, B.; Landt, M.; Kebernik, J.; Schwarz, B.; et al. Clinical bioprosthetic heart valve thrombosis after transcatheter aortic valve replacement. J. Am. Coll. Cardiol. Intv. 2017, 10, 686–697. [Google Scholar] [CrossRef] [PubMed]
- Liao, K.; Seifter, E.; Hoffman, D.; Yellin, E.L.; Frater, R.W.M. Bovine pericardium versus porcine aortic valve: Comparison of tissues biological properties as prosthetic valves. Artif. Organs 1992, 16, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Sellers, S.L.; Gulsin, G.S.; Zaminski, D.; Bing, R.; Latib, A.; Sathananthan, J.; Pibarot, P.; Bouchareb, R. Platelets: Implications in aortic valve stenosis and bioprosthetic valve dysfunction from pathophysiology to clinical care. J. Am. Coll. Cardiol. Basic Trans. Sci. 2021, 6, 1007–1020. [Google Scholar] [CrossRef]
- Galiñanes, M.; Matata, B.M. Protein nitration is predominantly mediated by a peroxynitrite-dependent pathway in cultured human leucocytes. Biochem. J. 2002, 367, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Matata, B.M.; Galiñanes, M. Peroxynitrite is an essential component of cytokine production mechanism in human leukocytes through modulation of NF-kB DNA-binding activity. J. Biol. Chem. 2002, 277, 2330–2335. [Google Scholar] [CrossRef] [Green Version]
- Kostyunin, A.E.; Yuzhalin, A.E.; Rezvova, M.A.; Ovcharenko, E.A.; Glushkova, T.V.; Kutikhin, A.G. Degeneration of bioprosthetic heart valves: Update 2020. JAHA 2020, 9, e018506. [Google Scholar] [CrossRef]
- El Husseini, D.; Boulanger, M.C.; Mahmut, A.; Bouchareb, R.; Laflamme, M.H.; Fournier, D.; Pibarot, P.; Bossé, Y.; Mathieu, P. P2Y2 receptor represses IL-6 expression by valve interstitial cells through Akt: Implication for calcific aortic valve disease. J. Mol. Cell. Cardiol. 2014, 72, 146–156. [Google Scholar] [CrossRef]
- Kaden, J.J.; Dempfle, C.E.; Grobholz, R.; Tran, H.T.; Kiliç, R.; Sarikoç, A.; Brueckmann, M.; Vahl, C.; Hagl, S.; Haase, K.K.; et al. Interleukin-1 beta promotes matrix metalloproteinase expression and cell proliferation in calcific aortic valve stenosis. Atherosclerosis 2003, 170, 205–211. [Google Scholar] [CrossRef]
- Gao, G.; Wu, Y.X.; Grunkemeier, G.L.; Furnary, A.P.; Starr, A. Durability of pericardial versus porcine aortic valves. J. Am. Coll. Cardiol. 2004, 44, 384–388. [Google Scholar] [CrossRef]
- Ganapathi, A.M.; Englum, B.R.; Keenan, J.E.; Smith, P.K.; Glower, D.D.; Hughes, G.C. Long-term survival after bovine pericardial versus porcine stented bioprosthetic aortic valve replacement: Does valve choice matter? Ann. Thorac. Surg. 2015, 100, 550–559. [Google Scholar] [CrossRef]
- David, T.E.; Armstrong, S.; Maganti, M. Hancock II bioprosthesis for aortic valve replacement: The gold standard of bioprosthetic valves durability? Ann. Thorac. Surg. 2010, 90, 775–781. [Google Scholar] [CrossRef]
- Khoo, J.P.; Davies, J.E.; Ang, K.L.; Galiñanes, M.; Chin, D. Differences in performance of five types of aortic valve prostheses: Haemodynamic assessment by dobutamine stress echocardiography. Heart 2013, 99, 41–47. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phase A | Phase B1 | Phase B2 | |||||
|---|---|---|---|---|---|---|---|
| Control CABG | Control Mechanical Prostheses | Biological Prostheses | Control CABG | Control Mechanical Prostheses | Biological Prostheses | ||
| PATIENTS (number) | 112 | 49 | 37 | 301 | 45 | 36 | 477 |
| Male—total no. (%) | 59 (52.3) | 37 (75.5) | 27 (77.1) | 175 (58.5) | 41 (91.1) | 25 (71.4) | 328 (68.8) |
| Age—yr, mean (SD) | 76.9 (11.0) | 69.4 (7.6) | 59.6 (12.1) | 74.8 (7.8) | 76.2 (5.8) | 70.7 (9.5) | 79.1 (7.4) |
| Diabetes mellitus—total no. (%) | 30 (26.8) | 19 (30.6) | 6 (17.1) | 89 (29.8) | 10 (22.2) | 12 (34.3) | 132 (27.9) |
| Hypertension—total no. (%) | 90 (80.4) | 41 (85.4) | 24 (68.6) | 251 (84.2) | 35 (79.6) | 23 (65.7) | 400 (84.9) |
| MI—total no. (%) | NR | 49 (100) | 1 (2.7) | 16 (5.4) | 45 (100) | 0 (0) | 36 (7.6) |
| NO donors—total no. (%) | 5 (4.5) | 4 (8.2) | 0 (0) | 11 (3.7) | NR | NR | 18 (3.8) |
| Statins—total no. (%) | 64 (57.1) | 33 (67.3) | 15 (40.5) | 174 (57.8) | NR | NR | 284 (59.5) |
| OAC—total no. (%) | 30 (26.8) | 5 (10.2) | 6 (16.2) | 43 (14.3) | NR | NR | 105 (22.0) |
| APT—total no. (%) | 48 (42.9) | 35 (71.4) | 7 (18.9) | 111 (36.9) | NR | NR | 238 (49.9) |
| SURGICAL DATA | |||||||
| Valve Surgery + CABG—total no. (%) | 14 (12.5) | NR | NR | NR | NR | NR | NR |
| Cross-clamp time—min | |||||||
| Median | NR | 36.6 | 48.6 | 43.2 | NR | NR | NR |
| IQR | 33.0–44.4 | 38.4–57.6 | 33.0–57.0 | ||||
| CPB time—min | |||||||
| Median | NR | 69.0 | 63.9 | 58.8 | NR | NR | NR |
| IQR | 60.6–75.6 | 52.2–72.6 | 44.4–72.0 | ||||
| Type of Prostheses | Phase A (n = 112) | Phase B1 (n = 301) | Phase B2 (n = 477) |
|---|---|---|---|
| Porcine Xenograft | 16 | 7 | 51 |
| Mosaic (stented) | 9 | 2 | 36 |
| Epic & Epic Supra (stented) | 2 | 0 | 11 |
| Hancock II (stented) | 1 | 5 | 0 |
| Shelhigh (stentless) | 2 | 0 | 0 |
| Freestyle (stentless) | 0 | 0 | 2 |
| O’Brien (stentless) | 1 | 0 | 2 |
| Bovine Pericardium | 96 | 267 | 426 |
| Perimount Magna & Magna Ease (stented) | 26 | 136 | 297 |
| Mitroflow (stented) | 67 | 32 | 111 |
| Trifecta (stented) | 0 | 25 | 0 |
| Solo (stentless) | 1 | 30 | 12 |
| Perceval (sutureless) | 0 | 22 | 0 |
| Sapien (TAVI) | 2 | 20 | 6 |
| Jena (TAVI) | 0 | 2 | 0 |
| Equine Pericardium | 0 | 22 | 0 |
| 3f (stentless) | 0 | 15 | 0 |
| Enable (sutureless) | 0 | 7 | 0 |
| Porcine Pericardium | 0 | 5 | 0 |
| CoreValve (TAVI) | 0 | 4 | 0 |
| Acurate neo/TF (TAVI) | 0 | 1 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galiñanes, M.; Casós, K.; Blasco-Lucas, A.; Permanyer, E.; Máñez, R.; Le Tourneau, T.; Barquinero, J.; Schwartz, S., Jr.; Bottio, T.; Roussel, J.C.; et al. Oxidative Stress in Structural Valve Deterioration: A Longitudinal Clinical Study. Biomolecules 2022, 12, 1606. https://doi.org/10.3390/biom12111606
Galiñanes M, Casós K, Blasco-Lucas A, Permanyer E, Máñez R, Le Tourneau T, Barquinero J, Schwartz S Jr., Bottio T, Roussel JC, et al. Oxidative Stress in Structural Valve Deterioration: A Longitudinal Clinical Study. Biomolecules. 2022; 12(11):1606. https://doi.org/10.3390/biom12111606
Chicago/Turabian StyleGaliñanes, Manuel, Kelly Casós, Arnau Blasco-Lucas, Eduard Permanyer, Rafael Máñez, Thierry Le Tourneau, Jordi Barquinero, Simo Schwartz, Jr., Tomaso Bottio, Jean Christian Roussel, and et al. 2022. "Oxidative Stress in Structural Valve Deterioration: A Longitudinal Clinical Study" Biomolecules 12, no. 11: 1606. https://doi.org/10.3390/biom12111606